Corpus callosum
| Brain: Corpus callosum | ||
|---|---|---|
 |
||
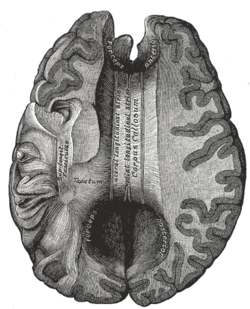
| Corpus callosum from above. (Anterior portion is at the top of the image.) | ||
 |
||
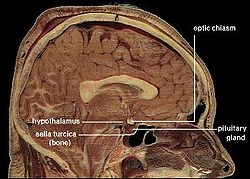
| Median sagittal section of brain (person faces to the left). Corpus callosum visible at center, in light gray. | ||
| Gray's | subject #189 828 | |
| NeuroNames | hier-173 | |
| MeSH | Corpus+Callosum | |
| NeuroLex ID | birnlex_1087 | |
The corpus callosum (Latin: tough body) is a wide, flat bundle of axons beneath the cortex in the eutherian brain at the longitudinal fissure. It connects the left and right cerebral hemispheres and facilitates interhemispheric communication. It is the largest white matter structure in the brain, consisting of 200–250 million contralateral axonal projections.
Contents |
Anatomy
The posterior portion of the corpus callosum is called the splenium; the anterior is called the genu (or "knee"); between the two is the truncus, or "body", of the corpus callosum. The part between the body and the splenium is often markedly thinned and thus referred to as the "isthmus". The rostrum the part of the corpus callosum that projects posteriorly and inferiorly from the anteriormost genu, as can be seen on the sagittal image of the brain displayed on the right. Anatomically, rostrum derives from the Latin for rooster, a reference to its resemblance to the crest of a rooster.
Thinner axons in the genu connect the prefrontal cortex between the two halves of the brain. Thicker axons in the midbody of the corpus callosum and in the splenium interconnect areas of the premotor and supplementary motor regions and motor cortex, with proportionally more corpus dedicated to supplementary motor regions. The posterior body of the corpus communicates somatosensory information between the two halves of the parietal lobe and visual center at the occipital lobe.[1] [2]
Evolution
The corpus callosum is absent in monotremes and marsupials, although it is generally present in mammals otherwise.[3] In primates, the speed of nerve transmission depends on its degree of myelination, or lipid coating. This is reflected by the diameter of the nerve axon. In most primates, axonal diameter increases in proportion to brain size to compensate for the increased distance to travel for neural impulse transmission. This allows the brain to coordinate sensory and motor impulses. However, the scaling of overall brain size and increased myelination has not occurred between chimpanzees and humans. This has resulted in the human corpus callosum requiring double the time for interhemispheric communication as a macaques.[1]
Sexual dimorphism
The corpus callosum and its relation to gender has been a subject of debate in the scientific and lay communities for over a century. Initial research in the early 20th century claimed the corpus to be different in size between men and women. That research was in turn questioned, and ultimately gave way to more advanced imaging techniques that appeared to refute earlier correlations. The new advent of physiologic based imaging has altered the paradigm dramatically, with the relationship between gender and the corpus callosum becoming a subject of almost exponentially increasing amounts of research in recent years.
Original studies and dispute
The first study of the corpus with relation to gender was by R. B. Bean, a Philadelphia anatomist, who suggested in 1906 that the "exceptional size of the corpus callosum may mean exceptional intellectual activity" and that there were measurable differences between men and women. Perhaps reflecting the political climate of the times, he went on to claim differences in the size of the callosum across different races. His research was ultimately refuted by Franklin Mall, the director of his own laboratory.[4]
Of more mainstream impact was a 1982 Science article by Holloway and Utamsing that suggested sex difference in human brain morphology which related to differences in cognitive ability.[5] Time published an article in 1992 which suggested that because the corpus is "often wider in the brains of women than in those of men, it may allow for greater cross-talk between the hemispheres—possibly the basis for women’s intuition."[6]
More recent publications in the psychology literature have raised doubt as to whether the anatomic size of the corpus is actually different. A meta-analysis of 49 studies since 1980 found that, contrary to de Lacoste-Utamsing and Holloway, no sex difference could be found in the size of the corpus callosum, whether or not account was taken of larger male brain size.[4] A study in 2006 using thin slice MRI showed no difference in thickness of the corpus when accounting for the size of the subject.[7]
Physiologic imaging and gender identity disorder
The ability to evaluate the form and function of the human mind has undergone almost exponential growth and a paradigm shift in recent years. Magnetic resonance imaging, for example, is now being used to analyze physiology in addition to anatomy. Using diffusion tensor sequences on MRI machines, the rate that molecules diffuse in and out of a specific area of tissue and different rates of metabolism can be measured. These sequences have found consistent sex differences in human corpus callosal morphology and microstructure.[8][9][10]
Morphometric analysis has also been used to study specific 3-dimensional mathematical relationships with MRIs, and have found consistent and statistically significant differences across genders.[11][12] Specific algorithms have found significant gender differences in over 70% of cases in one review. [13]
Research has been done on the shape of the callosum in those with gender identity disorder. Researchers were able to demonstrate that the shape of the corpus in men who felt they were female were actually reversed, and that the same held true for women who felt they were men. The publishers of this article argued that the shape of the corpus defined the mental sex of an individual over their physical sex.[13]
The relationship between the corpus callosum and gender remains an active subject of debate in the scientific and lay community.
Other correlations
The front portion of the corpus callosum has been reported to be significantly larger in musicians than non-musicians,[14] and to be 11% larger in left-handed and ambidextrous people than right-handed people.[15][16]
Epilepsy
The symptoms of refractory epilepsy can be reduced by cutting the corpus callosum in an operation known as a corpus callosotomy.[17] This is usually reserved for cases in which complex or grand mal seizures are produced by an epileptogenic focus on one side of the brain, causing an interhemispheric electrical storm. The work up for this procedure involves an electroencephalogram, MRI, PET scan and evaluation by a specialized neurologist, neurosurgeon, psychiatrist, and neuroradiologist before surgery can be considered.[18]
Pathology
- Alien hand syndrome
- Alexia without agraphia (seen with damage to splenium of corpus callosum)
- Agenesis of the corpus callosum.
- Split-brain
- Septo-optic dysplasia (deMorsier syndrome)
- Multiple sclerosis in which there is a classic lesion of the corpus callosum known as Dawson's fingers.
External links
- BrainMaps at UCDavis corpus callosum
- Comparative Neuroscience at Wikiversity
- NIF Search - Corpus callosum via the Neuroscience Information Framework
- National Organization for Disorders of the Corpus Callosum
References
- ↑ 1.0 1.1 Caminiti R, Ghaziri H, Galuske R, Hof PR, Innocenti GM. Evolution amplified processing with temporally dispersed slow neuronal connectivity in primates. Proc Natl Acad Sci U S A. 106:19551–19556. doi:10.1073/pnas.0907655106 PMID 19875694
- ↑ Hofar, F. and Frahm, J., Topography of the human corpus callosum revisited—Comprehensive fiber tractography using diffusion tensor magnetic resonance imaging. NeuroImage 32 (2006) 989-994
- ↑ Keeler, "Absence of the corpus callosum as a Mendelizing character in the house mouse." Proceedings of the National Academic of Sciences, 1936.|url=http://www.jstor.org/pss/86284
- ↑ 4.0 4.1 Bishop KM, Wahlsten D (1997). "Sex differences in the human corpus callosum: myth or reality?". Neurosci Biobehav Rev 21 (5): 581–601. doi:10.1016/S0149-7634(96)00049-8. PMID 9353793. http://linkinghub.elsevier.com/retrieve/pii/S0149-7634(96)00049-8.
- ↑ de Lacoste-Utamsing, C., Holloway, R. L. "Sexual dimorphism in the human corpus callosum." Science, 216, 1431–1432, 1982.
- ↑ C Gorman (20 January 1992). "Sizing up the sexes". Time: 36–43.
- ↑ Luders, Eileena; Narr, Katherine L.a; Zaidel, Eranb; Thompson, Paul M.a; Toga, Arthur W. Gender effects on callosal thickness in scaled and unscaled space. 17(11), 31 July 2006, pp 1103-1106
- ↑ Dubb A, Gur R, Avants B, Gee J (2003). "Characterization of sexual dimorphism in the human corpus callosum". Neuroimage 20 (1): 512–9. doi:10.1016/S1053-8119(03)00313-6. PMID 14527611. http://linkinghub.elsevier.com/retrieve/pii/S1053811903003136.
- ↑ Westerhausen R, Kreuder F, Dos Santos Sequeira S, et al. (2004). "Effects of handedness and gender on macro-and microstructure of the corpus callosum and its subregions: a combined high-resolution and diffusion-tensor MRI study.". Cognitive Brain Research 21 (3): 418–26. doi:10.1016/j.cogbrainres.2004.07.002. PMID 15511657. http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6SYV-4D2N0W6-1&_user=10&_coverDate=11%2F01%2F2004&_rdoc=18&_fmt=high&_orig=browse&_srch=doc-info(%23toc%234844%232004%23999789996%23525350%23FLA%23display%23Volume)&_cdi=4844&_sort=d&_docanchor=&view=c&_ct=18&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=285c939df34b6d6d8794ca92e4b87cda.
- ↑ Shin YW, Kim DJ, Ha TH, et al. (2005). "Sex differences in the human corpus callosum: diffusion tensor imaging study". Neuroreport 16 (8): 795–8. doi:10.1097/00001756-200505310-00003. PMID 15891572. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=0959-4965&volume=16&issue=8&spage=795.
- ↑ Kontos, Despina. Megalooikonomou, Vasileios. Gee, James C. Morphometric analysis of brain images with reduced number of statistical tests: a study on the gender-related differentiation of the corpus callosum. Artificial Intelligence in Medicine. 47(1):75-86, 2009 Sep.
- ↑ "Our results suggest that the problem of sexual dimorphism of the corpus callosum is very complex, because the identical variables (section surface area or its perimeter) do not exhibit the same behavior in males and in females, implicating that these variables even cannot be simply compared between the sexes." [official translation of abstract] (Serbian) G. Spasojević, Z. Stojanović, D. Suscević and S. Malobabić, "Sexual dimorphism of the human corpus callosum—digital morphometric study", Vojnosanitetski pregled 63/11 (2006): 933–938.
- ↑ 13.0 13.1 Yokota, Y. Kawamura, Y. Kameya, Y. Callosal Shapes at the Midsagittal Plane: MRI Differences of Normal Males, Normal Females, and GID. Annual International Conference of the IEEE Engineering in Medicine & Biology Society. 3:3055-8, 2005.
- ↑ Levitin, Daniel J. "This is Your Brain on Music", '
- ↑ Witelson SF (1985). "The brain connection: the corpus callosum is larger in left-handers". Science 229 (4714): 665–68. doi:10.1126/science.4023705.
- ↑ Driesen, Naomi R.; Naftali Raz (1995). "The influence of sex, age, and handedness on corpus callosum morphology: A meta-analysis". Psychobiology 23 (3): 240–247. http://www.psychonomic.org/search/view.cgi?id=1412.
- ↑ Clarke DF, Wheless JW, Chacon MM, et al. (2007). "Corpus callosotomy: a palliative therapeutic technique may help identify resectable epileptogenic foci". Seizure 16 (6): 545–53. doi:10.1016/j.seizure.2007.04.004. PMID 17521926.
- ↑ "WebMd Corpus Callotomy". July 18, 2010. http://www.webmd.com/epilepsy/corpus-callosotomy.
|
|||||||||||||||||||||||